
Percutaneous jejunostomy tubes (J tube)
Percutaneous jejunostomy tubes (J tube)
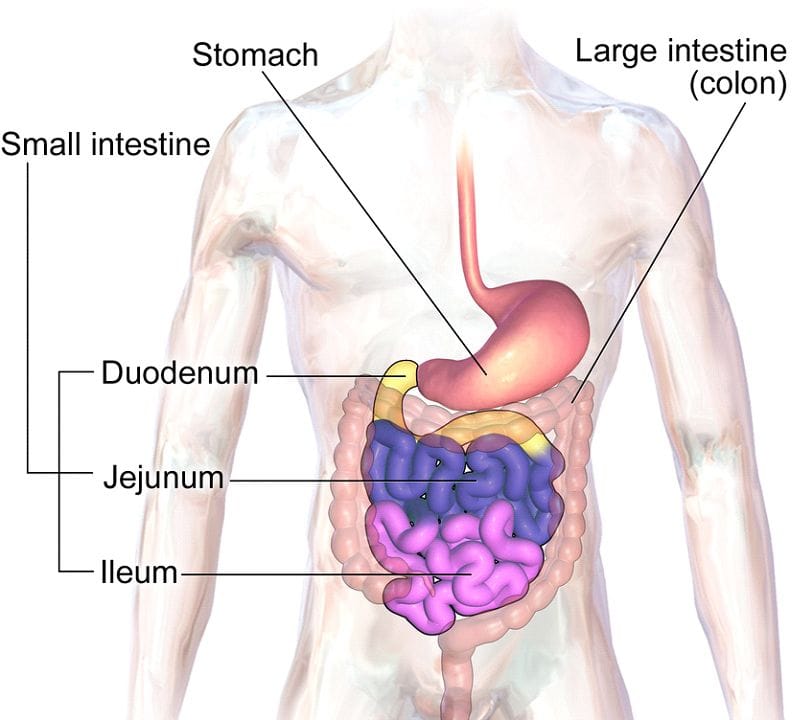
The gastrointestinal tract is a long connection that extends from the mouth to the anus. Food travels from the mouth, to the esophagus, to the stomach, to the small intestine, to the large intestine, and finally out through the anus. The small intestine is broken down into three parts: the duodenum, jejunum, and ileum.

Jejunostomy Tube
A jejunostomy tube is a device placed by a Surgeon in the operating room. It is used to give direct access to jejunum for feeding, hydration, and medications. Jejunostomy tubes are used to deliver feedings when the patient is unable to use their stomach for nutrition due to aspiration risk, motility problems, post operatively from surgeries that need complete stomach rest after or if the patient has some alteration in the anatomy of the GI tract. Although your jejunostomy tube is placed by a surgeon it can be exchanged by an interventional radiologist as needed. It can be removed in your doctors’ office at any point that you no longer need it.
Types of Jejunostomy (J) Tubes
Regular “MIC” J tube (see figure 2a)

Low Profile MIC-Key Button J tube (see figure 2b).

The Low profile J tube is only made by the company Avenos and not AMT. Placement of a low profile button tube is not recommended until your weight is stable. Until your weight is stable a regular MIC J tube with an adjustable stoma/retention disc is more appropriate. In order to have this type of tube you will need a measurement of your stoma size and the tube can be ordered and placed at your next exchange.
Figure 3. A picture demonstrating what a stoma size is.

Flushing the J Tube (this is extremely important to prevent clogging of your tube).
- Flush the J tube with at least 45-60 ml of water every 6 hours (even while the feeds are running).
- Flush with 45-60 ml water before and after any tube feeding.
- Flush with 45-60 ml water before, between and after any medications.
Administering Medications
- A J tube is very narrow and clogs easily so medications should only be given through your J tube if there is no other option.
- Try to get your medications in liquid form to try to keep your tube from clogging.
- For pills, check with your doctor or pharmacist before crushing any medications. If you are on a medication that is extended release then it should not be crushed.
- If your pills are in tablet form then crush the tablet well and mix with warm water to give the liquid mixture through your tube.
- Always give one medication at a time and give water in between each medication to prevent clogging.
- For capsules, check with your doctor or pharmacist before opening the capsule. Open and dissolve powder with enough water to make a liquid.
- Medications such as Flomax and Prilosec have little hard round pellets inside the capsule and these will clog your tube. Contact your doctor to change these medications to an alternative.
- Flush your J tube with 45 ml water before you give medications. If the tube is sluggish stop and put papaya enzyme into the tube to improve the flow BEFORE putting medications.
- Flush your J tube with at least 45 ml of water between medications and after medications.
Pump Feedings
- Jejunal (J) tube feedings should be given via a feeding pump.
- Jejunal (J) tubes are not appropriate for bolus feeds and you likely will not tolerate them if given by bolus.
- A pump should have been arranged for you with home health and the home health nurse should have given you instructions on how to use the pump.
- Flush your J tube with 45-60 ml water before feeds, every 6 hrs while they are running and any time the feeds are held to prevent your tube from clogging.
- If your pills are in tablet form then you will need to crush the tablet well and mix with warm water to give through your tube.
- Do not give more than 1-2 medications at a time to prevent clogging the tube.
Dislodgement
Try to replace the tube into the opening about 1-2 inches and tape the tube to your abdomen. Then call your care team. DO NOT USE THE TUBE.
Leaking
- A small amount of leaking around the G tube is normal. You can apply a dressing at the Gastrostomy tube site if there is drainage.
- Most times when the G tube site is leaking it is from the external bumper/ retention disc having loosened. This happens from the gauze being placed under the disc and slides the disc up. You may notice your home health nurse place the gauze under the disc since nurses used to be taught to do that, however, it is no longer recommended. Check the disc daily and if it has slid up away from the skin gently slide the disc back down until it is against the skin. This usually will fix the leakage.
- Other times, the tube site can leak if the tube got pulled on forcefully accidentally and the site gets stretched out. With good skin care keeping the skin as dry as possible and with good nutrition the site will heal.
- You may hear someone mention “upsizing” the tube or making it larger if the site is leaking. This will actually make the problem worse and is not recommended.
Skin or excess tissue growing where the tube enters skin
- This is called granulation tissue, which is the body’s natural response to the tube. It is normal for this tissue to bleed a little when bumped or irritated. Call your care team to discuss treatment. This is not an emergency but should be addressed in a timely manner. Your provider can use silver nitrate sticks at the site to treat this.
J tube is sluggish
- If you notice you are having to push a bit harder to flush your tube this is when you should intervene. Do NOT wait until it is completely clogged or you may need to go back to the provider that placed the tube to have it exchanged.
- You can use papaya enzyme from your local vitamin store to help the flow through your tube. Take two tabs and crush them and mix them in warm water. Instill this mixture into the tube and leave it in the tube for 1-2 hours and flush with warm water after.
G tube completely clogged
- Once the tube is completely clogged your options may be limited so it is important to intervene before it completely clogs.
- If it is clogged you can try to slowly push /pull warm water in and out of the tube to try to break up a clog. Do not push hard forward or you may rupture the clogged tube. Never put any object into the tube to unclog it. If you are unable to unclog the tube, call your provider to arrange to have the tube exchanged.
Call your doctor and seek immediate medical care if you notice the following signs and symptoms:
- Signs of infection
- Increase pain, swelling, warmth, redness around drain site
- Pus draining from the insertion site
- Fever
- Sudden change in color and smell of your drainage.
- Tube is coming loose out of your insertion site.
- The site is leaking excessively and you have already checked the disc and slid it down if needed.
- Your tube is clogged and you are unable to unclog it.
- Your tube is broken.